-

Membranous nephropathy
Membranous nephropathy– a kidney disease
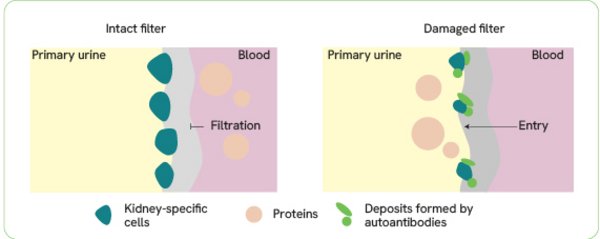
Membranous nephropathy (MN, also membranous glomerulonephritis) is a chronic inflammatory kidney disease. It has been known for many years that deposits form in the kidneys during the course of this disease. These deposits impair the kidney function and lead to inflammation. Despite intensive research, the exact causes remained unknown for a long time. In 2009, the first antibody was discovered that causes the damaging deposits in the more common form of the disease – primary membranous nephropathy (pMN) – and subsequently disrupts kidney's filtering function. It is an autoantibody, which means that it is an antibody directed against the structures of the body itself.
 |
symptoms of pMN are
-
proteinuria (excessive excretion of proteins with the urine),
-
hyperlipidaemia and lipiduria (disorders of the blood lipid metabolism),
-
formation of oedema (fluid accumulation in the tissues).
The disease can vary in severity, ranging from spontaneous improvement to persistent proteinuria or complete kidney failure.
Autoantibodies and primary membranous nephropathy
In 2009, researchers identified the first autoantibody involved in the development of pMN in the blood of MN patients. It is directed against the PLA2R (phospholipase A2 receptor) protein, which is found in the cells of the kidney’s blood-urine filter. The anti-PLA2R antibodies accumulate in this area, forming deposits that destroy the cells and impair the kidney’s filtering function. The discovery of anti-PLA2R autoantibodies is considered a milestone in nephrological research. They can be found in the blood of 70 % to 80 % of patients.
Further research in 2014 revealed a second autoantibody targeting the THSD7A (thrombospondin type-1 domain-containing 7A) protein, which is found in the kidney. It can be detected in the blood of approximately 3 % to 5 % of pMN patients who do not have antibodies against PLA2R.
In 2020, a third autoantibody was finally identified: It is directed against the podocyte antigen NELL1 (neural epidermal growth factor-like 1 protein). Anti-NELL1 antibodies are found in patients with pMN who have tested negative for anti-PLA2R and anti-THSD7A antibodies. Depending on the study, its prevalence in kidney biopsy samples ranges between 5 % and 16 %. Further studies are needed to investigate the role of anti-NELL1 antibodies in greater detail and to characterise them more accurately.
Forms of membranous nephropathy
In addition to primary membranous nephropathy, there is also a secondary form of the disease. This condition, known as secondary membranous nephropathy (sMN), develops as a result of another underlying disease, such as an infection, an autoimmune disease, a tumour or drug poisoning. Approximately 20 % to 30 % of MN patients suffer from the secondary form. No corresponding autoantibodies have been detected in these patients to date.
The diagnostic differentiation between primary and secondary MN is crucial for the choice of therapy: While the treatment of sMN primarily focuses on the underlying disease, pMN can usually be successfully treated with immunosuppressants.
In some patients, no disease-causing autoantibodies or other identifiable causes can be found so far. This form of MN is referred to as idiopathic.